




ChannelDynamics
Measure the performance of your sales force and marketing channels, adapt your commercial strategy and gain real world competitive insights.












The second article in the two-part series builds on the country-level analysis, investigating more detailed trends around gender and specialty. As pharma and life sciences companies face an evolving landscape for interacting with healthcare systems, these articles set out to inject clarity in a complex promotional environment.
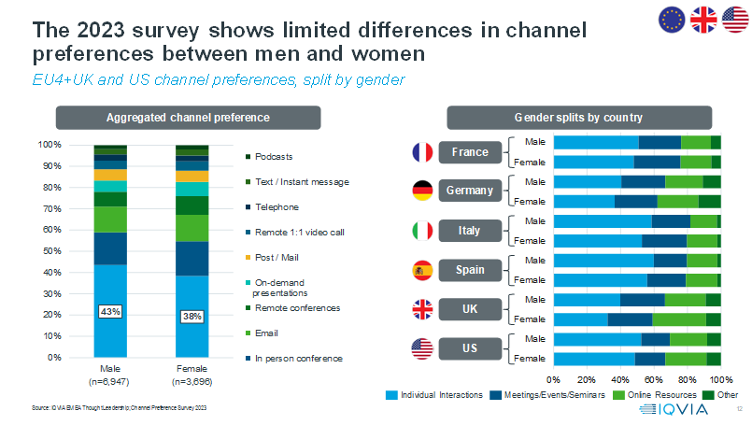
Closer investigation of channel preferences between genders shows limited differences. Across the US, EU4+UK there is a 5% difference with respect to 1:1 F2F visits, with men showing a 43% preference share and women 38% for this channel. Breaking the analysis down by country also shows similarities between genders within a country. However, the size of these gender differences dwindles when compared to the differences between countries, so an HCP’s location remains the most important factor to consider when choosing a suitable engagement strategy.
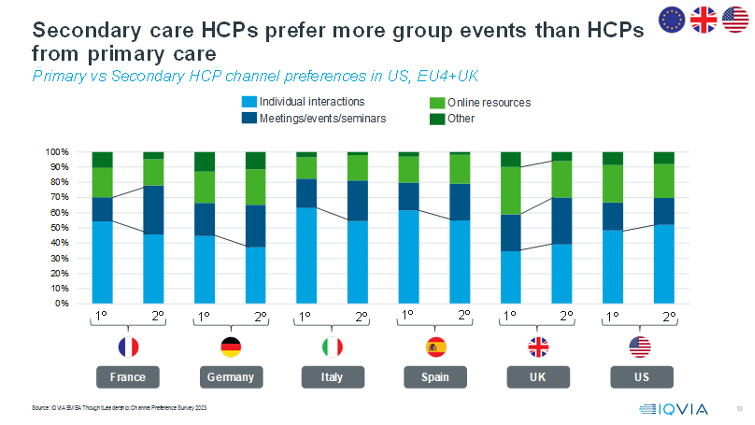
Across the EU4+UK and US, secondary care HCPs prefer a 6% lower share of 1:1 F2F visits than primary care HCPs. Instead, secondary care HCPs prefer in-person conferences, which have an 18% share of channel preference. Podcasts and text/instant messaging channels are the least popular, with a 2% average share in both primary and secondary settings. Diving deeper into the different specialties, it is clear the desire for emails is fairly consistent, but anaesthetists stand out as having the lowest preference for individual interactions and meetings.

When the specialty analysis is distilled further at a country level, more subtle nuances come to the fore. In France and the UK, the preference for meetings and seminars is more pronounced in secondary care, whilst in Germany, Italy and Spain it is the preference for individual interactions in primary care that is most noticeable. The US and the UK are the only countries where individual interactions are more popular in secondary than primary care.
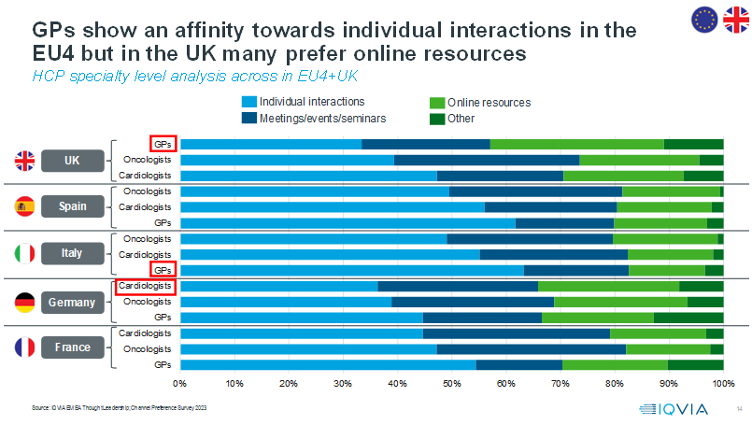
Adding a further level of granularity to examine three specialties across each country in the EU4+UK, GPs in Italy show a 63% preference for individual interactions whereas GPs in the UK are almost half that figure at 33% and Germany split the difference with a 45% share. Cardiologists least prefer individual interactions of the German specialties in scope, showing a higher relative affinity towards meetings and seminars of 29%. Oncologists in the UK and France are the only specialties to show a greater preference for meetings and seminars at 34% and 35% respectively.
Are these preferences being reflected in the interactions that HCPs are currently having with industry? Matching the 2023 channel preference data to actual reported interactions, at an HCP level, reveals whether HCPs are receiving information via their ideal mix of channels. In Italy and Spain, HCP preferences and actual interactions are well-aligned, largely due to their greater preference for F2F engagement. Those in the UK and Germany show less alignment, 34% and 40% respectively. The disparity is predominantly caused by a mismatch between emails, F2F visits and postal mailings, as well as the lower affinity for F2F interactions in these countries.
When looking at the alignment at a specialty level across the EU4+UK, there is an even greater variation in alignment between the received and preferred channel mix. HCPs working in trauma, ENT specialists and dermatologists show a high degree of alignment whereas nurses, haematologists and oncologists sit at the other end of the spectrum, with up to 60% of these HCPs not receiving their preferred channel mix.

Taking a step back, we can compare the relative importance of the four factors that were assessed during the 2023 Channel Preference Survey. The country in which an HCP works is the most important factor to consider with respect to channel mix. There are significant differences in preferences between countries, attributable to a combination of geographical factors, regulation, cultural influence and historical expectations (i.e., engaging with HCPs via the channel they are accustomed to and well-acquainted with). Within each country, it is also useful to take into account an HCP’s specialty. For example, GPs in the UK have the lowest preference for individual interactions of any group in the major markets surveyed. Variations of this kind highlight the challenges with accessing HCPs in different care settings across countries, as well as the differences in how specialties are dealing with increased workloads and patient backlogs from a healthcare systems perspective. The third most important consideration is age – there are generational differences in how HCPs prefer to engage with industry. The younger generation of ‘digital native’ HCPs, born after 1980, are more likely to have the necessary skills and willingness to engage with digital platforms and social media. Their preferences will become even more significant in future years as they gradually replace the retiring older generation of ‘digital immigrant’ HCPs. Gender is the least significant factor when choosing an optimal channel mix – HCP’s preferences are more heavily impacted by the aforementioned factors.
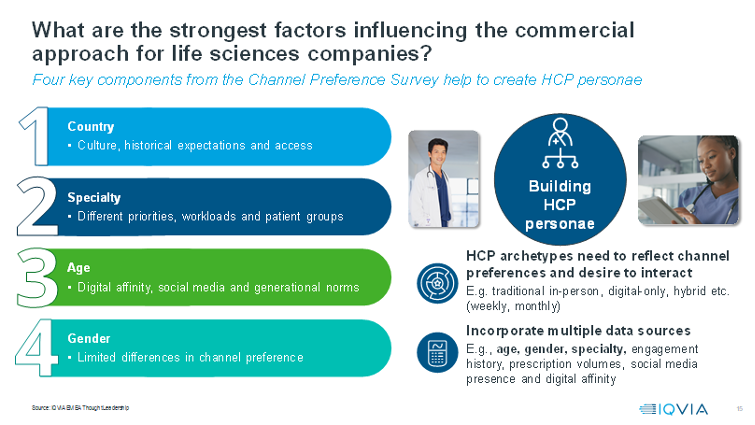
Ideally, pharma and life sciences companies should consider all available information about an HCP when determining the optimal engagement strategy at an individual level. A useful approach would be to integrate information about an HCP’s country, specialty, age and gender from multiple sources to build an HCP persona. These personae can also include the HCP’s engagement history and their desired frequency of different types of interactions. Ultimately, the goal is to use data, analytics and insights to profile HCP archetypes which will help to guide an optimal channel mix and engagement approach, orchestrated in line with HCP preferences.
If you have missed the first part of the blog, read it here.
Measure the performance of your sales force and marketing channels, adapt your commercial strategy and gain real world competitive insights.
Maximize the value of your brand with personalized, precise, and efficient communications.
Take advantage of the latest tools, techniques, and deep healthcare expertise to create scalable resources, precision insights, and actionable ideas.