












Payers
Greater visibility into the impact of treatments.
In support of National Kidney Month this March, IQVIA is helping to raise public awareness by sharing data-driven insights on patient access in chronic kidney disease (CKD). CKD is a disorder in which the kidneys are damaged to the extent that patients cannot filter blood as well as they should. It is a common disease and a leading cause of death in the United States. Many patients who suffer from this disease remain undiagnosed or untreated, subsequently costing the U.S. healthcare system billions of dollars annually.
CKD by the Numbers1
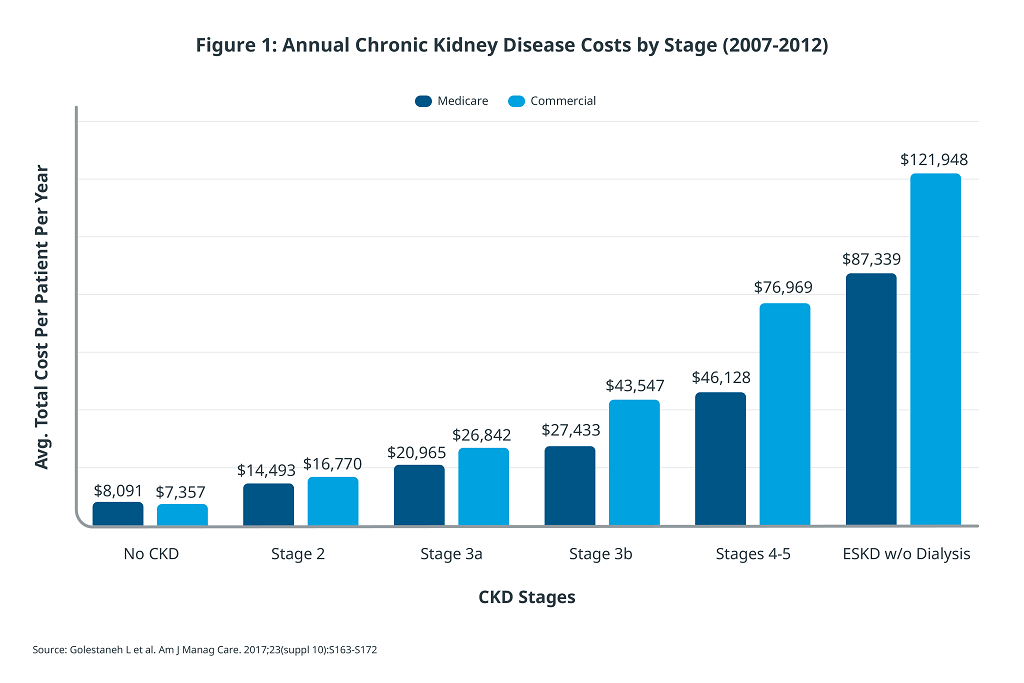
As patients progress through stages of chronic kidney disease, the annual cost of treatment increases substantially. Stage 2 CKD patients, on average, require roughly double the treatment costs of non-CKD patients. For patients in End-Stage Kidney Disease (ESKD) without dialysis, the cost of treatment is more than 10 times of those with CKD. Earlier diagnosis and treatment not only lead to better quality of life for patients, but also reduce the overall cost of treatment by slowing disease progression.4
For many patients, high blood pressure and diabetes lead to heightened risk of developing CKD and escalated overall healthcare costs. For patients under the age of 65 with both CKD and T2D, the cost of treatment can be as much as 60% higher than treating T2D alone, while having a meaningful impact on quality of life.5 Despite the known correlations and higher annual treatment costs, there remain many gaps in care for patients. This causes substantial portions of the population to remain undiagnosed.
According to the CDC, 9 out of 10 adults with CKD do not know they have CKD.6 Inequities and disparities in awareness, testing, diagnosis, and intervention may be more prominent at certain points in the patient journey. For instance, Native American, Black, and Hispanic patients have high rates of diabetes,7 which increases the risk of developing CKD.8
By 2060, the diabetes population in the U.S. is expected to double to over 60 million patients,9 with up to 40%10 also suffering from CKD, many of whom will remain undiagnosed. Building and investing in treatment protocols, supporting patient organizations, and more is needed to bridge known health disparities and the overall undertreatment of CKD. Utilizing IQVIA’s Longitudinal Access and Adjudication Data (LAAD), a recent analysis of CKD in T2D treatments, Kerendia (finerenone) and SGLT2is, showed that 94% of diabetes patients who are also diagnosed with CKD are not gaining access to such newer therapies indicated to reduce risks of renal and cardiovascular outcomes associated with CKD, and are thus, not benefitting from available treatments.11
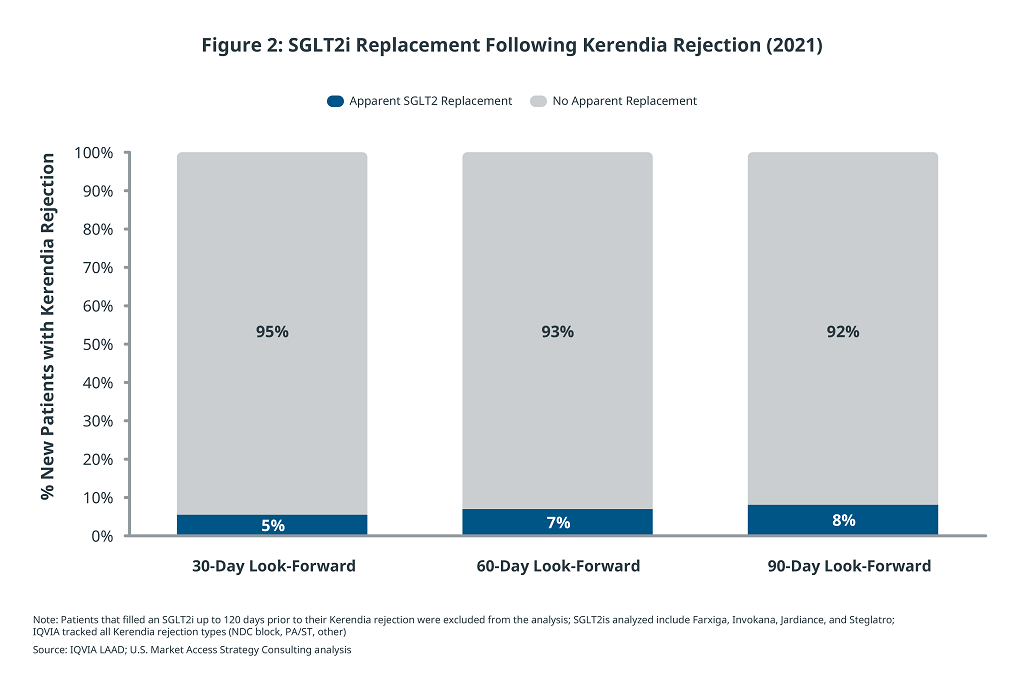
The IQVIA analysis also demonstrated that 35% of all Kerendia new-to-brand patients – and only 29% of Medicare Part D patients – were able to fill their prescriptions and begin therapy. The largest obstacle preventing these patients from obtaining treatment was payer access control, which more than half of patients were unable to overcome. The impact of payer restrictions was observed across all payer channels, including Medicare Part D and Commercial, which includes private insurance through employers and the healthcare exchanges. Analyzing patients not already on an SGLT2i, IQVIA determined that more than 90% of patients who initially received a payer rejection for Kerendia were not subsequently treated with an SGLT2i as an alternative within a 90-day period.11 Therefore an unintended consequence of payer controls may not only be a delay in treatment but a lack of intervention overall.
CKD is a costly disease for patients, payers, and society as a whole. As patients progress through the stages of the disease, annual cost of treatment increases while quality of life declines. Despite the known linkages between T2D and CKD, up to 90% of patients remain undiagnosed. Within minority populations, where chronic disease prevalence is even higher, there remains a gap in the journey to treatment. Given the progressive and irreversible nature of CKD, there is a clear population health need for early diagnosis and treatment. Analysis of payer controls, however, indicates that access barriers are a necessary factor for consideration when addressing this need.
Once patients have navigated the healthcare system to treatment, there are additional barriers faced in payer coverage which can have unintended consequences. In a disease area where untreated patients will face a heightened risk of disease progression, the balance of patient access and healthcare costs is particularly crucial.
The authors would like to thank several IQVIA colleagues for their support. This includes but is not limited to, Eric Savage and Madeline Andres. The authors would also like to acknowledge Bayer for sponsoring the analyses used in this blog. The findings and final editorial decisions belong to IQVIA.
Sources
1. Centers for Disease Control and Prevention. Accessed January 31, 2022. https://www.cdc.gov/kidneydisease/basics.html
2. Wu B, Bell K, Stanford A, et al. Understanding CKD among patients with T2DM: prevalence, temporal trends, and treatment patterns–NHANES 2007-2012. BMJ Open Diabetes Res Care. 2016;4(1):e000154
3. Papademetriou V, Nylen ES, Doumas M, et al. Chronic kidney disease, basal insulin glargine and health outcomes in people with dysglycemia: the ORIGIN study. Am J Med. 2017;12(130):1465.e27-1465.e39
4. Golestaneh L, Alvarez PJ, Reaven NL, et al. All-cause costs increase exponentially with increased chronic kidney disease stage. Am J Manag Care. 2017;23(suppl 10):S163-S172
5. United States Renal Data System. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2019
6. Centers for Disease Control and Prevention. Accessed August 16, 2021. https://www.cdc.gov/kidneydisease/pdf/Chronic-Kidney-Disease-in-the-US-2021-h.pdf
7. Centers for Disease Control and Prevention. Accessed August 16, 2021. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
8. National Institute of Diabetes and Digestive and Kidney Diseases. Accessed August 16, 2021. https://www.niddk.nih.gov/health-information/diabetes/overview/preventing-problems/diabetic-kidney-disease
9. Lin J, Thompson TJ, Cheng YJ, et al. Projection of the future diabetes burden in the United States through 2060. Popul Health Metr. 2018;16(1):9.
10. Bailey RA, Wang Y, Zhu V, Rupnow MFT. Chronic kidney disease in US adults with type 2 diabetes: an updated national estimate of prevalence based on Kidney Disease: Improving Global Outcomes (KDIGO) staging. BMC Res Notes. 2014;7:415
11. IQVIA Longitudinal Access & Adjudication Data analysis of Kerendia and SGLT2 usage among Type II diabetes patients diagnosed with CKD (based on anonymized January 2020 – December 2021 pharmacy and medical claims).
Greater visibility into the impact of treatments.
See how we partner with organizations across the healthcare ecosystem, from emerging biotechnology and large pharmaceutical, to medical technology, consumer health, and more, to drive human health forward.