-
Americas

-
Asia & Oceania

-
A-I
J-Z

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
Regions
-
Americas
-
Asia & Oceania
-
Europe
-
Middle East & Africa
-
Americas
-
Asia & Oceania
-

Europe
Europe
- Adriatic
- Belgium
- Bulgaria
- Czech Republic
- Deutschland
- España
- France
- Greece
- Hungary
- Ireland
- Israel
- Italia
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
SOLUTIONS
-
Research & Development
-
Real World Evidence
-
Commercialization
-
Safety & Regulatory Compliance
-
Technologies
LIFE SCIENCE SEGMENTS
HEALTHCARE SEGMENTS
- Information Partner Services
- Financial Institutions
- Public Health and Government
- Patient Associations
- Payers
- Providers
THERAPEUTIC AREAS
- Cardiovascular
- Cell and Gene Therapy
- Central Nervous System
- GI & Hepatology
- Infectious Diseases and Vaccines
- Oncology
- Pediatrics
- Rare Diseases
- View All

Impacting People's Lives
"We strive to help improve outcomes and create a healthier, more sustainable world for people everywhere.
LEARN MORE
Harness the power to transform clinical development
Reimagine clinical development by intelligently connecting data, technology, and analytics to optimize your trials. The result? Faster decision making and reduced risk so you can deliver life-changing therapies faster.
Research & Development OverviewResearch & Development Quick Links

Real World Evidence. Real Confidence. Real Results.
Generate and disseminate evidence that answers crucial clinical, regulatory and commercial questions, enabling you to drive smarter decisions and meet your stakeholder needs with confidence.
REAL WORLD EVIDENCE OVERVIEWReal World Evidence Quick Links

See markets more clearly. Opportunities more often.
Elevate commercial models with precision and speed using AI-driven analytics and technology that illuminate hidden insights in data.
COMMERCIALIZATION OVERVIEWCommercialization Quick Links

Service driven. Tech-enabled. Integrated compliance.
Orchestrate your success across the complete compliance lifecycle with best-in-class services and solutions for safety, regulatory, quality and medical information.
COMPLIANCE OVERVIEWSafety & Regulatory Compliance Quick Links

Intelligence that transforms life sciences end-to-end.
When your destination is a healthier world, making intelligent connections between data, technology, and services is your roadmap.
TECHNOLOGIES OVERVIEWTechnology Quick Links
CLINICAL PRODUCTS
COMMERCIAL PRODUCTS
COMPLIANCE, SAFETY, REG PRODUCTS

BLOGS, WHITE PAPERS & CASE STUDIES
Explore our library of insights, thought leadership, and the latest topics & trends in healthcare.
DISCOVER INSIGHTSTHE IQVIA INSTITUTE
An in-depth exploration of the global healthcare ecosystem with timely research, insightful analysis, and scientific expertise.
SEE LATEST REPORTS



FEATURED INNOVATIONS
-
IQVIA Connected Intelligence™
-
IQVIA Healthcare-grade AI™
-
Human Data Science Cloud
-
IQVIA Innovation Hub
-
Decentralized Trials
-
Patient Experience powered by Apple
WHO WE ARE
- Our Story
- Our Impact
- Commitment to Public Health
- Code of Conduct
- Environmental Social Governance
- Privacy
- Executive Team
NEWS & RESOURCES


Unlock your potential to drive healthcare forward
By making intelligent connections between your needs, our capabilities, and the healthcare ecosystem, we can help you be more agile, accelerate results, and improve patient outcomes.
LEARN MORE
IQVIA AI is Healthcare-grade AI
Building on a rich history of developing AI for healthcare, IQVIA AI connects the right data, technology, and expertise to address the unique needs of healthcare. It's what we call Healthcare-grade AI.
LEARN MORE
Your healthcare data deserves more than just a cloud.
The IQVIA Human Data Science Cloud is our unique capability designed to enable healthcare-grade analytics, tools, and data management solutions to deliver fit-for-purpose global data at scale.
LEARN MORE
Innovations make an impact when bold ideas meet powerful partnerships
The IQVIA Innovation Hub connects start-ups with the extensive IQVIA network of assets, resources, clients, and partners. Together, we can help lead the future of healthcare with the extensive IQVIA network of assets, resources, clients, and partners.
LEARN MORE
Proven, faster DCT solutions
IQVIA Decentralized Trials deliver purpose-built clinical services and technologies that engage the right patients wherever they are. Our hybrid and fully virtual solutions have been used more than any others.
LEARN MORE
IQVIA Patient Experience Solutions powered by Apple
Empowering patients to personalize their healthcare and connecting them to caregivers has the potential to change the care delivery paradigm. IQVIA and Apple are collaborating to bring this exciting future of personalized care directly to devices patients already have and use.
LEARN MOREWORKING AT IQVIA
Our mission is to accelerate innovation for a healthier world. Together, we can solve customer challenges and improve patient lives.
LEARN MORELIFE AT IQVIA
Careers, culture and everything in between. Find out what’s going on right here, right now.
LEARN MORE
WE’RE HIRING
"Improving human health requires brave thinkers who are willing to explore new ideas and build on successes. Unleash your potential with us.
SEARCH JOBSBlog
CGRP inhibitors: the first designer drugs for migraine
Dec 21, 2018
Introduction
Migraine is a common neurological condition that is characterized by highly incapacitating, recurrent, primary headaches that can last for 4 to 72 h. The typical manifestation of migraine headaches includes debilitating throbbing pain around the eyes and temples that is often unilateral and pulsating in nature, and is accompanied by photophobia, osmophobia, nausea, emesis, loss of appetite and sometimes perceptual disturbances called aura. More than 90% of patients with migraine are unable to work or function normally during their migraine attacks. According to the World Health Organization’s 2012 global burden of disease figures, migraine is ranked in the top 40 conditions causing worldwide disability, above all other neurological disorders other than stroke, meningitis and epilepsy. It is the third most prevalent illness in the world, affecting 39 million in the USA and 1 billion worldwide. Migraine disproportionately affects women – 18% of women, 6% of men and 10% of children experience migraine.
Patients experience migraine episodes which are often volatile. In some patients, migraine is related with allodynia or specific triggers increasing the susceptibility to migraine attack. Some of the factors that potentially trigger migraine attacks include stress, environmental stimuli like weather or bright lights, hormonal fluctuations in women, hunger, too little or too much sleep, dietary elements (wine, caffeine, monosodium glutamate, artificial sweeteners, nitrates) and odors (perfumes, cigarette smoke).
The trigeminovascular pathway: role of CGRP in migraine
Over the past 300 years, migraine pathophysiology has been dominated by two main theories – the vascular theory and the central neuronal theory. Based on vascular theory, vasoconstrictors such as ergotamine and the triptans have been conventionally used for migraine management. However, during the 1980s, evidence emerged that bolstered the involvement of neuronal mechanism and the central role of trigeminal ganglion and calcitonin gene-related peptide (CGRP), a vasoactive neuropeptide, in primary headache pathogenesis. Migraine triggers are likely to cause primary brain dysfunction, which cause cranial vasodilation and mechanical activation of trigeminal sensory nerve fibers. Neuronal excitability of cerebral cortex and trigeminal nucleus leads to a pain response that is conveyed to the brainstem and evokes release of vasoactive peptides including CGRP from trigeminal fibers. These peptides exacerbate vasodilation, neuronal inflammation and transmission of central nociception. Based on this mechanism, recent prophylactic therapies, which include either CGRP receptor antagonists (the gepants), or monoclonal antibodies (mAbs) to CGRP or its receptor, have evolved that cause functional blockade of CGRP release into the cranial venous outflow for acute and chronic migraine management.
Migraine management
There are 2 broad approaches for managing chronic migraine: non-pharmacological approach with lifestyle and trigger management, and pharmacological approach including acute treatments (medications taken during attacks or exacerbations of chronic pain) and preventive treatments (medications designed to reduce the tendency to have attacks). The pharmacological approaches are listed in Table 1.
| Line of Treatment | Acute Treatment | Prophylactic Treatment |
|---|---|---|
| First-line | NSAIDs Triptans |
Beta Blockers Angiotensin blockers Tricyclics |
| Second-line | Ergot derivatives | Anticonvulsants |
| Third-line | N/A | Anti-CGRP therapies |
Table 1: Acute and prophylactic treatments for migraine
Anti-CGRP therapies: the first designer drugs for migraine
As enlisted in Table 1, antiepileptics, antidepressants and antihypertensives, that were originally not developed for migraine prevention have been used as off-label drugs to prevent or reduce migraine attacks. Several of these prophylactic medications have intolerable side effects, must be taken daily and are associated with variable efficacy. The CGRP inhibitors make up the first drug class developed specifically for migraine headache. There are 2 different classes of drugs inhibiting CGRP to prevent migraine: monoclonal antibodies (mAbs) and small molecule CGRP receptor antagonists (gepants).
CGRP inhibitor mAbs for migraine management
mAbs represent an attractive prospect for migraine treatment as they have a long half-life that make them suitable to act on chronic migraine attacks. Moreover, they can be designed to have precise, long duration of activity that prevents frequent dosing, e.g. once or twice monthly thereby increasing patient compliance and reducing side effects. In addition, antibodies are highly specific, allowing them to have highly selective targeting of either CGRP or its receptor.
There are two types of CGRP inhibitor mAbs:
- those that bind directly to the CGRP ligand and block its binding to the receptor
- those binding and exerting a competitive, reversible blockade of the CGRP receptor
Small molecule anti-CGRP drugs for migraine management
Soon after the role of CGRP in migraine was elucidated in molecular pathology studies, small molecule “gepants” were the first class of anti-CGRP drugs that were investigated for migraine. The initial products demonstrated a reduction in pain compared with placebo, but further development was discontinued in lieu of incidence of hepatotoxicity. After nearly a decade, the development of the gepant class has resumed, with a next-generation of agents that do not produce the metabolites implicated in causing hepatotoxicity.
The landscape of anti-CGRP therapies that are in active development for migraine, as depicted in Figure 1, includes three marketed products, four in phase III evaluation, one in phase I evaluation and one in preclinical evaluation.
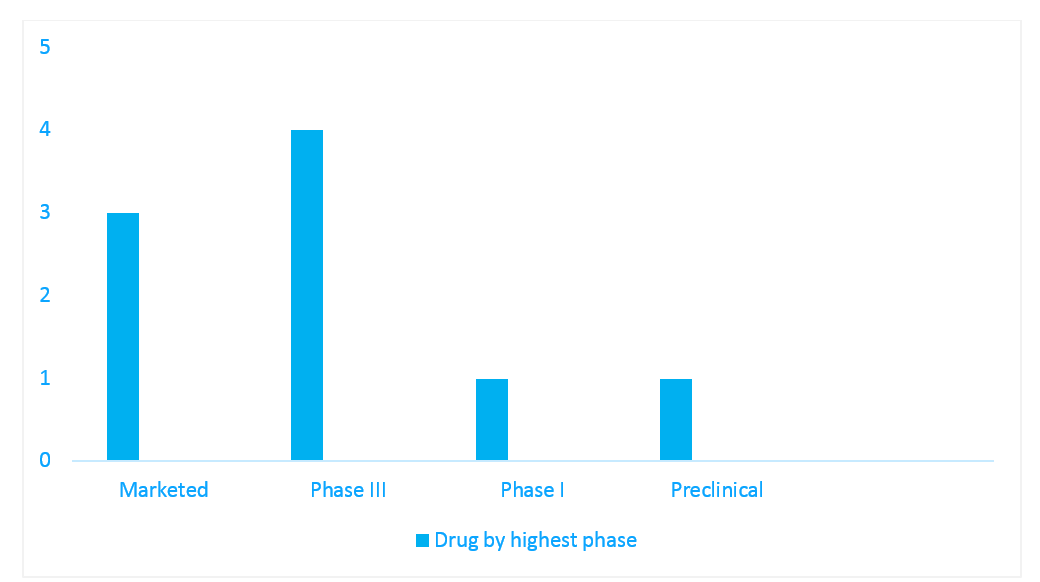
Figure 1: Pipeline snapshot of anti-CGRP therapies in active development for migraine, per highest phase
Source: IQVIA Pipeline Intelligence
Conclusion
Most of the patients who have a migraine attack begin by treating themselves with over-the-counter medications. None of the other medications used in clinical practice earlier were specifically designed for the prevention of migraine. The advent of the CGRP inhibitors heralds a paradigm shift in the treatment armamentarium for migraine. Antagonists of the CGRP pathway, especially mAbs, have proven to be efficacious and safe preventative therapies for episodic and chronic migraine in clinical trials, however, more real-world evidence is warranted as there is an absence of long-term experience with this class. CGRP and its receptors are widely prevalent in both the vasculature, and in the peripheral and central nervous system, and are involved in several physiological processes. Therefore, blocking CGRP may pose a risk in patients with comorbidities such as cardiovascular diseases. Mild injection-site pain, pruritus and erythema were the common adverse events reported in patients treated with the CGRP inhibitor mAbs. There are also no head-to-head comparison trials between these drugs to hand-pick the most efficacious and safe CGRP inhibitor for migraine management.
A draft evidence report from Institute for Clinical and Economic Review (ICER) concluded that while CGRP inhibitors are projected to have a positive impact on the health of patients with chronic or episodic migraines for whom earlier preventive therapies have failed relative to no treatment, it is likely that the inhibitors will exceed willingness-to-pay thresholds per quality-adjusted life year (QALY) in the general population. ICER also found that treatment with CGRP inhibitors resulted in higher total costs, more migraine-free days and increased QALYs compared with no preventive treatment, in both chronic and episodic migraine in patients who failed prior treatments. In conclusion, given the high cost of these mAbs, physicians should identify patients who are responding well to conventional therapies and adhere to these medications; CGRP inhibitors should be reserved as a frontline treatment option for patients with refractory migraine episodes in whom prior preventive therapies have failed.
Register to the INNsight Newsletter for regular updates on pipeline intelligence.